
Across the U.S., two powerful trends are colliding: the housing stock is getting older, and so are the people living in it. Many clients dream of “aging in place” in the homes and neighborhoods they know best—but those same homes often come with steep repair bills, poor accessibility, and hidden safety risks. For occupational therapists working in home safety and modifications, this “aging home crisis” is not just a challenge; it is a defining opportunity for our profession.
The Double Burden of Old Homes and Limited Budgets
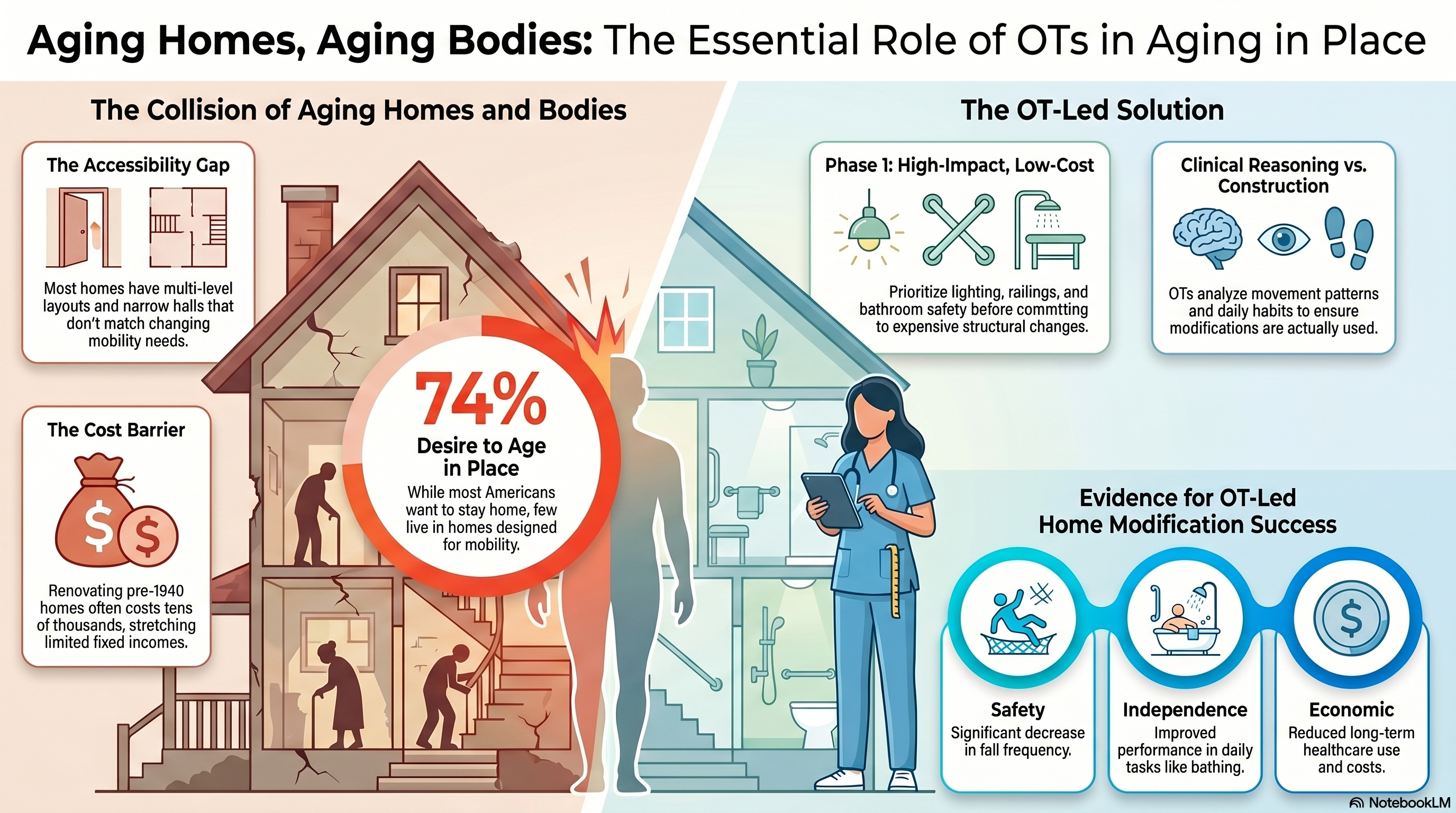
Older homes can be beautiful—think original hardwoods, charming staircases, and historic details—but they often hide expensive problems. Aging roofs, outdated plumbing and wiring, narrow doorways, and small bathrooms all add cost and complexity when a client needs accessibility changes. Renovating a pre-1940 home can quickly reach tens of thousands of dollars, especially once structural or systems issues appear mid-project—an especially tough reality for older adults living on fixed incomes.
OTs who practice in home accessibility live in this tension every day: clients want to stay, the home needs work, and the budget is finite. Our role is to help families prioritize what truly matters for safety and independence, rather than chasing a perfect (and often unaffordable) “forever home” remodel.
The Accessibility Gap: Homes That Don’t Match Changing Bodies
While many older adults live with mobility limitations, relatively few live in homes designed with those limitations in mind. Multi-level layouts, internal steps, narrow halls, and bathrooms without grab bars or curbless showers are common—not only in older homes, but also in many “standard” suburban houses built in the last several decades. Research on aging in place and indoor accessibility has repeatedly shown that when essential rooms (bedroom, bathroom, kitchen) are on different levels, and when steps and narrow spaces are common, older adults are more likely to relocate as their mobility changes.
On the other hand, relatively modest structural changes—such as creating one-level living, adding railings and grab bars, improving lighting, and removing trip hazards—are associated with better function and a higher likelihood of remaining at home. These are exactly the types of changes occupational therapists are trained to design and prioritize.
What the Evidence Says About OT-Led Home Modifications
Recent systematic reviews of home modifications for aging in place confirm what many clinicians see every day: when OTs lead home safety and accessibility interventions, falls decrease, functional independence improves, and quality of life goes up. Evidence-based programs that combine individualized assessment, client-centered goal setting, and targeted home changes can also reduce health care use and costs over time.
Yet the literature also points to important gaps:
- We need more personalized, occupation-focused intervention research rather than “one size fits all” home checklists.
- We need to better understand how smart-home technologies (from lighting and sensors to remote monitoring and voice controls) can be integrated into safe, realistic plans for older adults.
- We need longer-term follow-up to see how well modifications work years down the line as health and abilities change.
These gaps map directly onto the skills and creativity that home accessibility OTs already bring to the table.
The OT Mindset: Beyond Grab Bars and Gadgets
Contractors and builders are essential partners in home modifications—but they are not a replacement for occupational therapy. OTs are uniquely trained to analyze the interaction between person, environment, and occupation: how an individual’s body, habits, roles, and priorities intersect with their physical space and daily routines.
That means:
- We start with occupations and goals, not products. What does “staying home” actually look like for this person? Is it bathing independently, cooking one meal a day, managing pet care, or safely getting to the mailbox?
- We match modifications to real movement patterns. Instead of installing generic equipment, we observe transfers, mobility, vision, cognition, and sensory factors—and then design the space around those specific abilities and risks.
- We balance safety with dignity and identity. A grab bar or ramp that a client feels embarrassed to use is not truly functional. OTs are trained to negotiate aesthetics, stigma, and family dynamics alongside safety.
In older homes where every inch counts, this level of clinical reasoning can mean the difference between a costly, underused remodel and a focused, effective plan that clients truly adopt.
Working Within Real-World Constraints
One of the hardest parts of home modification practice is working inside real constraints: fixed incomes, rental agreements, homeowners’ association rules, and contractors’ timelines. Clients read headlines about six-figure renovations and assume that if they cannot afford a full remodel, they cannot safely age in place at all.
OTs can reframe that story by:
- Prioritizing “Phase 1” changes that drastically reduce fall risk: entry and exit, stairs, bathroom safety, and primary pathways.
- Identifying low-cost, high-impact modifications first (for example, improved lighting, contrast, railings, and strategic furniture rearrangement) while planning for larger structural changes over time.
- Helping clients and families decide when “modify” is best—and when “move” is the safer and more cost-effective path, based on function, prognosis, and home feasibility.
This phased, clinical approach is especially important in older homes where unexpected issues can quickly blow up a DIY project or a contractor’s initial estimate.
Why Systems Are Calling for More OTs in Home & Community Practice
Policy and payment trends are beginning to catch up with what OTs already know: safe, accessible housing is a core health issue. Medicare home safety evaluations, fall-related quality measures, HUD grants for older adult home modifications, Medicaid home- and community-based services (HCBS), and public health fall-prevention initiatives are all pointing toward greater investment in home safety and aging in place.
These shifts create clear opportunities for occupational therapists to:
- Partner with health systems, housing agencies, and community organizations around home safety programs.
- Develop specialized roles and businesses focused on fall prevention, accessibility consulting, and universal design for aging in place.
- Use advanced training—such as the Certified Home Accessibility Therapist (CHAT) credential—to deepen skills in construction literacy, building codes, and interdisciplinary collaboration.
As more seniors try to adapt 40–80-year-old homes to walkers, wheelchairs, and caregivers, the need for OTs who can bridge clinical practice and the built environment will only grow.
Changing Lives, One Older Home at a Time
The clash between aging homes and aging bodies is not going away. In fact, it may be one of the most important long-term trends shaping occupational therapy practice in home and community settings. Our profession is uniquely positioned to help clients and families see beyond quick fixes and product catalogs toward thoughtful, staged plans that keep people safely at home in the places they love.
When we combine our expertise in function and participation with a solid understanding of housing, construction, and universal design, we do more than prevent falls—we protect identity, relationships, and community connection. That is the heart of aging in place, and it is where occupational therapy shines the brightest.
Reference List
American Occupational Therapy Association. (2020). Occupational therapy practice framework: Domain and process (4th ed.). American Journal of Occupational Therapy, 74(Suppl. 2), 7412410010.
Harvard Joint Center for Housing Studies. (2019). Housing for an aging population. https://www.jchs.harvard.edu
Qian, Q. K., Ho, W. K. O., Jayantha, W. M., & Chan, E. H. W. (2022). Aging-in-place and home modifications for urban regeneration. Land, 11(11), 1956. https://doi.org/10.3390/land11111956
Realtor.com. (2026, April 2). The oldest homes in these 3 U.S. cities create a double burden for buyers and owners. In Realtor.com News & Insights. Realtor.com. https://www.realtor.com/news/trends/old-homes-construction-aging-expensive-repairs/
Realtor.com. (2025, November 19). 74% of Americans want to age in place, but are their homes ready? In Realtor.com Home Improvement. Realtor.com. https://www.realtor.com/advice/home-improvement/age-in-place-home-prepartions-renovations/
U.S. Census Bureau. (2023). Aging-ready homes in the United States: Perception versus reality (P23-219). U.S. Department of Commerce. https://www.census.gov/content/dam/Census/library/publications/2023/demo/p23-219.pdf
Wang, Z., & colleagues. (2025). A systematic review of home modifications for aging in place in older adults. [Journal title], [volume(issue)], [page range]. https://doi.org/10.XXXX/%5Bdoi-number%5D
Airgood-Obrycki, W., & Molinsky, J. (2020). Accessibility features for older households in subsidized housing. Cityscape, 22(3), 95–128.
Granbom, M., Iwarsson, S., Kylberg, M., Pettersson, C., & Slaug, B. (2016). A public health perspective to environmental barriers and accessibility problems for senior citizens living in ordinary housing. BMC Public Health, 16, 772. https://doi.org/10.1186/s12889-016-3411-9
Szanton, S. L., Thorpe, R. J., Boyd, C., Tanner, E. K., Leff, B., Agree, E., Guralnik, J., & Gitlin, L. N. (2015). Community Aging in Place, Advancing Better Living for Elders: Preliminary findings from a pilot study. Journal of Applied Gerontology, 34(1), NP3–NP25. https://doi.org/10.1177/0733464812463984
Leave a Reply