
Chronic kidney disease (CKD) and kidney failure are placing growing pressure on health systems, families, and homes. As more older adults live long enough to require dialysis, and as home-based treatment becomes more common, the home is increasingly being asked to function as a site of complex medical care rather than simply a place of recovery. This shift has important implications for occupational therapists (OTs), particularly those with expertise in home assessment, accessibility, caregiver support, and environmental modification.
Home dialysis is often promoted as a more flexible, person-centered alternative to in-center treatment, and growing registry data suggest it is gaining traction in both the United States and Europe. Yet the success of home dialysis depends on much more than medical suitability alone. Patients and caregivers must integrate equipment, storage, infection control, treatment routines, and emergency preparedness into everyday life at home, often while managing frailty, mobility limitations, visual impairment, fatigue, and caregiver burden. For that reason, the increasing use of dialysis at home strengthens the case for OT involvement in home modification and functional planning.
Why this issue is growing
The need for dialysis is closely tied to the burden of CKD, and that burden is rising in older adults. Reviews focused on home dialysis in older populations note that the number of older adults receiving dialysis has increased over time, reflecting both population aging and improved survival with chronic disease. This trend matters because older adults on dialysis are also more likely to have coexisting impairments that affect balance, endurance, cognition, hand function, transfers, and the ability to manage multi-step medical routines independently.
At the same time, home dialysis use has increased in several settings. U.S. data summarized from the United States Renal Data System show that home dialysis among incident patients rose substantially over the last decade, increasing from roughly 8 percent to over 13 percent. European data similarly describe home dialysis as a cost-effective and person-centered modality that has received renewed attention in recent years, even if uptake still varies by country. Taken together, these trends suggest that more medically complex care is moving into residential settings.
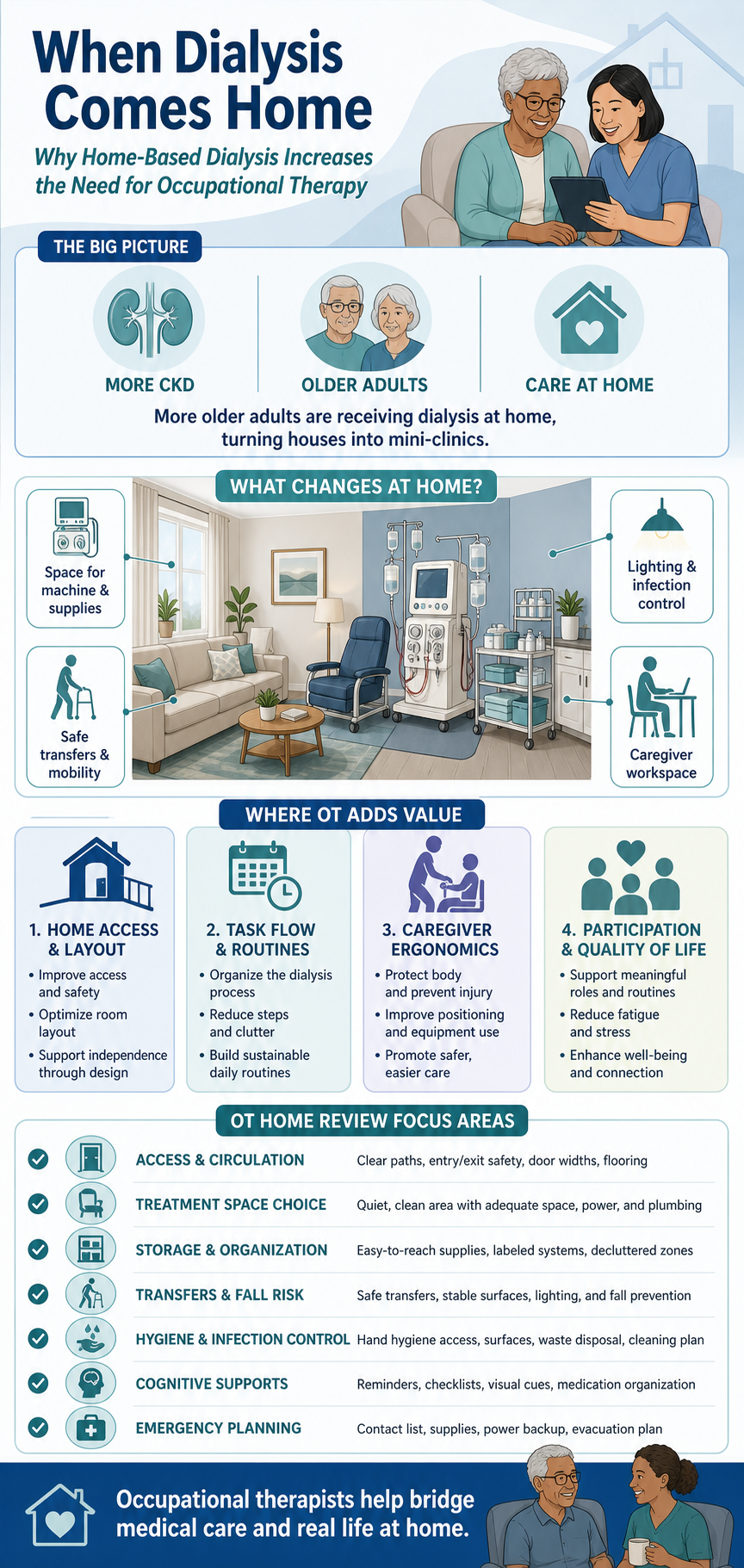
That shift is not merely logistical. It changes what the home must do. A home that once needed to support bathing, cooking, sleeping, and leisure may now also need to accommodate a dialysis machine, water-related requirements or supplies, treatment seating or bed positioning, infection control procedures, safe lighting for line management, medication organization, and enough room for caregivers to assist without injury. In practical terms, the home becomes part clinic, part storage area, part caregiving workspace, and part refuge. Making those roles coexist safely is fundamentally an occupational and environmental challenge.
What the qualitative evidence shows
One of the most useful sources for understanding this issue is the recent systematic review of qualitative research on barriers and facilitators to home hemodialysis. Unlike outcome studies focused on mortality, hospitalization, or cost, qualitative studies explore how patients, caregivers, and clinicians experience home treatment in real life. That perspective is especially valuable for occupational therapists because the main concerns are often not purely medical; they are environmental, functional, emotional, and relational.
The review supports several themes that are highly relevant to OT practice. First, patients and families often describe the physical demands of fitting treatment into the home. Limited space for machines and supplies, concern that the home will begin to feel like a hospital, and difficulty integrating treatment areas into ordinary living routines are recurring barriers. These concerns directly support the argument that home layout, storage planning, accessibility, and environmental adaptation matter to the feasibility of home dialysis.
Second, the review highlights the burden placed on caregivers. Home hemodialysis can shift significant responsibilities onto partners or family members, including setup, monitoring, troubleshooting, lifting, organizing supplies, and responding to unexpected events. For older households, where a spouse may also have arthritis, impaired vision, or their own chronic illness, those demands are not minor. The qualitative evidence therefore supports a broader systems view in which successful home dialysis depends not just on the patient, but on the functional capacity of the household.
Third, the review identifies facilitators that align well with OT intervention. Patients are more likely to succeed when they receive robust training, dependable technical support, clear routines, and confidence-building preparation for emergencies. Although nephrology teams lead the dialysis education itself, OTs are well positioned to translate complex treatment routines into practical daily habits within the specific realities of a person’s home, body, and caregiver situation.
What this article does and does not support
The qualitative systematic review does support the thesis that as home dialysis expands, the home environment becomes a critical determinant of treatment success. It also supports the idea that environmental barriers, caregiver strain, and the challenge of integrating medical treatment into daily life are central issues rather than side notes. Those findings make the article a strong foundation for an evidence-based blog about why home-based dialysis increases the need for professionals who understand function and environment.
However, the article does not explicitly study occupational therapy or formal home modification services. It also does not quantify how many patients need modifications, which types of modifications are most common, or whether OT involvement improves dialysis outcomes directly. To make the case for OTs more explicitly, it is helpful to pair this dialysis-specific review with broader home-modification research showing that OT-led, client-centered environmental interventions improve daily activity performance and can reduce hazards and caregiver strain in older adults.
Why OT is a logical response
Occupational therapy has long been concerned with the fit between a person’s abilities, daily occupations, and environment. When a necessary activity becomes harder because the space is poorly organized, physically inaccessible, cognitively confusing, or unsafe, the problem is not located in the person alone. It is located in the interaction between person, task, and environment. Home dialysis is a vivid example of that interaction.
A client may be medically cleared for home hemodialysis yet still struggle if the home has poor lighting for visualizing tubing, inadequate circulation space for a caregiver to assist, unsafe transfer routes to the treatment chair, no reliable storage plan for supplies, or too many interruptions for a long multi-step procedure. Likewise, a person using peritoneal dialysis may need support for hygiene routines, workspace setup, hand function, fatigue management, and emergency planning around daily occupations. These are areas where OTs add value by combining clinical reasoning, environmental analysis, and practical adaptation.
Research on home modification outside the dialysis literature strengthens this point. Client-centered home modifications have been associated with improved performance in daily activities and sustained benefits over time in older adults. OT guidance in home environments is also commonly linked to fall prevention, safer mobility, improved occupational performance, and reduced caregiver burden, all of which are highly relevant when life-sustaining treatment is delivered in the home. The evidence does not need to be dialysis-exclusive to be persuasive; it shows that OTs already have an established role in making homes safer and more functional for complex daily living.
Areas for OT focus in a home dialysis review
An OT evaluating a home for a client who requires in-home dialysis can bring a broader lens than a simple accessibility checklist. The goal is not only to determine whether treatment can fit into the home, but whether it can be carried out safely, consistently, and with the least possible disruption to health, function, and quality of life.
1. Access and circulation
The OT can assess how the client and any caregiver move from the home’s entrance to the treatment area, bathroom, kitchen, and bedroom. Narrow pathways, thresholds, clutter, poor flooring transitions, and low lighting may increase fall risk before or after treatment, especially for fatigued or hypotensive patients. Adequate turning radius and room for caregiver assistance are also important if the client uses a walker, wheelchair, or transfer aids.
2. Treatment space selection
The dialysis area must support safe positioning, privacy, comfort, visibility, and routine. Important questions include whether the client can reach and observe necessary equipment, whether there is enough stable surface area for supplies, whether the seating or bed setup supports posture and pressure management, and whether the environment allows sustained treatment without excessive interruption. The OT can help identify whether a bedroom, den, living room, or other space is best suited to this purpose.
3. Storage and organization
Home dialysis often requires substantial storage for supplies, consumables, and backup materials. The OT can assess whether storage is accessible, protected from contamination, logically arranged for workflow, and realistic for the client’s strength, balance, and memory. Poor storage design can create both safety hazards and treatment errors, especially when households are small or already crowded.
4. Transfer safety and mobility during and after treatment
Many dialysis clients are older adults with deconditioning, neuropathy, orthostatic symptoms, or balance limitations. The OT should assess transfers to and from the treatment chair or bed, route safety to the bathroom, need for grab bars or raised seating, and whether fatigue after treatment changes mobility demands. A home that is manageable at baseline may become risky immediately after dialysis.
5. Infection control and hygiene routines
While nephrology teams determine clinical protocols, OTs can help translate them into workable routines in the home. This may include evaluating handwashing access, cleanable surfaces, location of waste disposal, sequencing of setup and cleanup tasks, and the compatibility of the treatment area with pets, children, and normal household traffic. The practical question is whether the home supports adherence to safe habits without placing unrealistic demands on the patient or caregiver.
6. Cognitive load and routine management
Home dialysis can involve many repeated steps, alarms, and monitoring tasks. OTs can assess whether the client has memory, attention, executive function, visual-perceptual, or health-literacy challenges that interfere with safe self-management. Interventions might include visual cueing systems, simplified layouts, checklists, labeling, stepwise task sequencing, and environmental prompts.
7. Caregiver ergonomics and burden
Qualitative research repeatedly shows that caregiver burden is a key issue in home hemodialysis. OTs can examine whether caregivers must lift awkwardly, bend repeatedly, reach overhead for supplies, stand for prolonged periods, or manage tasks in cramped spaces. Reducing strain through better layout, equipment placement, seating, or workflow can improve sustainability for the whole household.
8. Emergency preparedness
The home review should also consider how the patient and caregiver would respond to alarms, bleeding, dizziness, loss of power, or the need to summon help. The OT can assess access to phones, visibility of emergency instructions, path clearance for first responders, and whether the client can safely terminate or pause routines as instructed by the medical team. Emergency planning is both a medical and environmental issue.
9. Participation and quality of life
Finally, OT should look beyond the mechanics of treatment. If dialysis supplies occupy the dining room, the family may lose a gathering space. If treatment timing eliminates valued activities, the client’s sense of identity may narrow to that of a patient. If the home feels permanently clinical, emotional well-being may decline. OT can help preserve meaningful roles and routines by minimizing environmental intrusion and supporting a better balance between treatment and ordinary life.
A practical thesis for clinicians and readers
The strongest evidence-based argument is not that every dialysis patient needs extensive remodeling. Rather, it is that the expansion of home dialysis in an aging population makes the fit between person, treatment, caregiver, and home environment increasingly consequential. When care shifts home, environmental barriers that were once inconvenient can become clinically significant. A poor transfer setup can increase falls; inadequate storage can undermine adherence; a confusing workflow can increase caregiver burden and treatment anxiety.
That is why OTs with expertise in home modification represent an important but under-recognized part of home dialysis success. Their contribution is not limited to recommending grab bars or rearranging furniture. It includes analyzing routines, preserving occupational participation, adapting the environment to reduce risk, supporting caregivers, and helping households absorb medical technology without losing function or dignity. In a health system that increasingly depends on the home to deliver complex care, that expertise is likely to become more valuable, not less.
Closing perspective
The literature supports a clear conclusion: dialysis needs are growing in older adults, home dialysis is receiving increasing attention and use, and the success of treatment at home depends heavily on the physical and social environment. The qualitative systematic review on barriers and facilitators to home hemodialysis is therefore a strong source for illustrating how treatment reshapes the home and household. When combined with evidence on OT-led home modification and functional assessment, it provides a credible foundation for arguing that OTs have a critical role in helping clients make home dialysis safer, more manageable, and more compatible with everyday life.
References
Charnow, J. (2021). Home dialysis use on theupswing. Renal & Urology News. Retrieved from: https://www.renalandurologynews.com/news/home-hemodialysis-and-peritoneal-dialysis-adoption-increasing-in-the-us/
Earley, Á., Lydon, S., Walker, R. C., Gannon, L., Reddan, D., Durack, L., & O’Connor, P. (2025). A Systematic Review of the Qualitative Research on Barriers and Facilitators to Home Hemodialysis. Hemodialysis international. International Symposium on Home Hemodialysis, 29(4), 434–441. https://doi.org/10.1111/hdi.13266
Jacquet, S., & Trinh, E. (2019). The Potential Burden of Home Dialysis on Patients and Caregivers: A Narrative Review. Canadian journal of kidney health and disease, 6, 2054358119893335. https://doi.org/10.1177/2054358119893335
Slon-Roblero, M. F., Stel, V. S., Sanchez-Alvarez, E., Manrique Escola, J., Fraga Dias, B. J., Auñón, A. S., Ferraro, P. M., De Meester, J. M., Boyer, A., Rydell, H., Hommel, K., Åsberg, A., Rama Arias, I., Methven, S., Espigares Huete, M. J., Abrahams, A. C., Palsson, R., Goffin, E., Aresté-Fosalba, N., Bello, A. J., … Kramer, A. (2026). Trends in home dialysis over the last decade in Europe: an ERA Registry study. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association – European Renal Association, 41(3), 457–475. https://doi.org/10.1093/ndt/gfaf171
Stark, S., Landsbaum, A., Palmer, J. L., Somerville, E. K., & Morris, J. C. (2009). Client-centred home modifications improve daily activity performance of older adults. Canadian journal of occupational therapy. Revue canadienne d’ergotherapie, 76 Spec No(Spec No), 235–245. https://doi.org/10.1177/000841740907600s09
USRDS (2023) Annual Report: End Stage Renal Disease: Chapter 2 Home Dialysis. Retrieved from: https://usrds-adr.niddk.nih.gov/2023/end-stage-renal-disease/2-home-dialysis
Witten, B. (2023). Home dialysis in the 2022 United States Renal Data system annual data report. Retrieved from: https://homedialysis.org/news-and-research/blog/526-home-dialysis-in-the-2022-united-states-renal-data-system-annual-data-report
Wu, H. H. L., Dhaygude, A. P., Mitra, S., & Tennankore, K. K. (2022). Home dialysis in older adults: challenges and solutions. Clinical kidney journal, 16(3), 422–431. https://doi.org/10.1093/ckj/sfac220
Leave a Reply